

Surgery
There are many gynecologic ailments that can be addressed surgically. Understanding your surgery is critical to your recovery and in obtaining informed consent. During our preoperative discussion, many points will be brought to your attention. This page revisits these topics in case you may have questions.
Major Surgeries

Minor Surgeries


Surgery Risks
Any surgery carries risks. We take every precaution to minimize surgical risks, but it is important to understand the risks involved with your procedure. Below is a general, but comprehensive list of surgical risks.
- Damage to surrounding structures (uterus, cervix, vagina, ovaries, fallopian tubes, bladder, bowel, nerves and blood vessels)
- Bleeding, possibly resulting in need for a blood transfusion or emergency hysterectomy (as a last resort)
- Failure to achieve the desired outcome
- Need for additional procedures if complication arises
- Wound infection
- Pain due to scarring
- Formation of a blood clot that can migrate to the lungs (pulmonary embolus)
- Formation of an abnormal connection between pelvic organs (fistula)
- In laparoscopy or hysteroscopy, there may be the need to convert to a traditional abdominal incision
- In hysteroscopy, there may be electrolyte imbalance requiring overnight admission or there may be perforation of the uterus requiring laparoscopy
Types of Traditional Incisions & Surgical Approaches
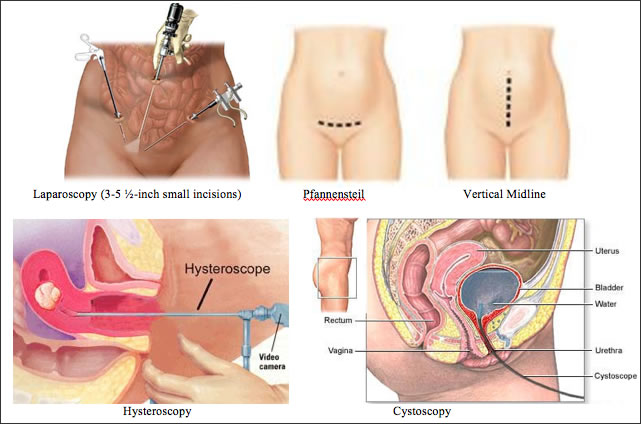
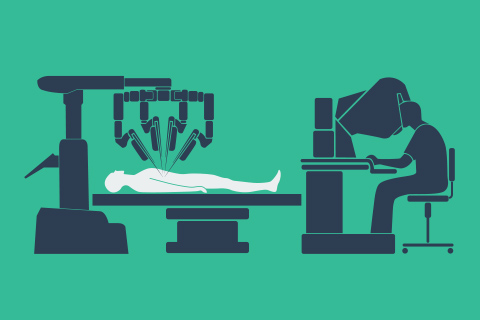
Robotic surgery using the da Vinci Surgical System:
Robotic surgery is a specific type of minimally invasive laparoscopic approach utilizing the da Vinci Surgical system robot, which the surgeon controls from a separate console. Benefits to robotic surgery include significantly less pain, a shorter hospital stay, faster return to normal daily activities – as well as the potential for better clinical outcomes. Furthermore, with the da Vinci surgical system, the minimally invasive capabilities exceed that of traditional laparoscopy.

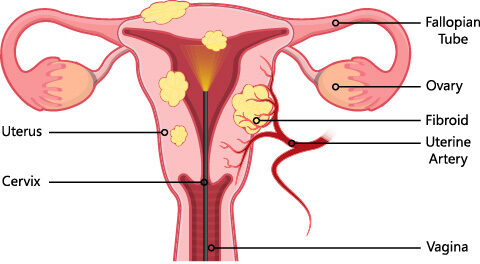
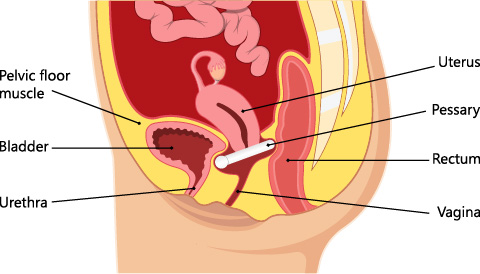
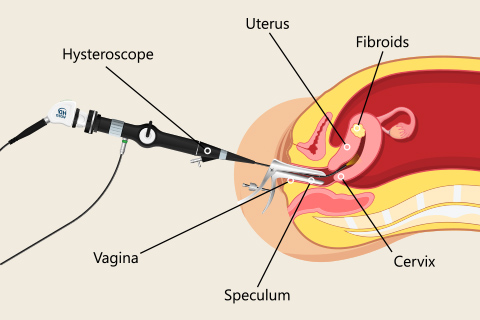
Generally, robotic surgery is used for surgical management of fibroids, pelvic organ prolapse, endometriosis and pelvic pain, and for hysterectomy. Below briefly gives pictorial examples of the above situations. Your surgeon will discuss your diagnosis in detail.

Pre-operative
A preop visit will be scheduled within the upcoming days to weeks before your surgery to answer last-minute questions and sign consents. Do not eat/drink anything after midnight the evening before your procedure. Avoid aspirin products and herbal remedies for 7 days preoperatively.
Please be at the hospital 2 hours before or at the surgery center 1 hour before your surgery time. We encourage you to bring your headphones and listen to music or equivalent to help relax you while you are waiting in the preop area.
Post-Operative Expectations for Recovery and Timeline
Recovery will depend on surgery being performed. In general, narcotics can cause constipation. It is recommended that you maintain stool softeners (Colace, Senokot) and a high fiber diet post-operatively while taking narcotics.
- For most laparoscopic procedures, expect a 1-2 week recovery. With robotic surgery you can expect discharge on the same day or the morning after surgery. Recovery is generally 2-3 weeks depending on the surgery performed.
- Total laparoscopic hysterectomy patients may return to work in 2-3 weeks with light activity restrictions and should abstain from vaginal intercourse for 4-6 weeks. Laparoscopic supracervical hysterectomy patients may return to work in 1-2 weeks with light activity restrictions and abstaining from intercourse for 3 weeks.
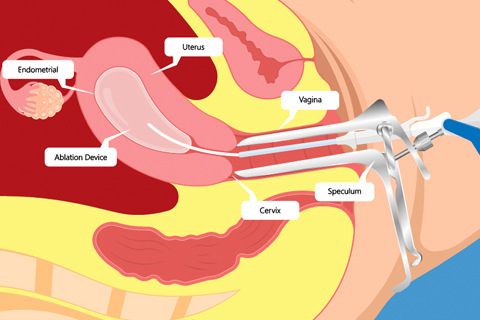
- Hysteroscopy and sterilization patients can return to work the next day. If you undergo an endometrial ablation, expect a watery vaginal discharge for approximately 3 weeks and a return to work 24 to 48 hours post operatively. Occasionally, at 6-8 weeks post-op from an endometrial ablation you may see bleeding equivalent to a period.
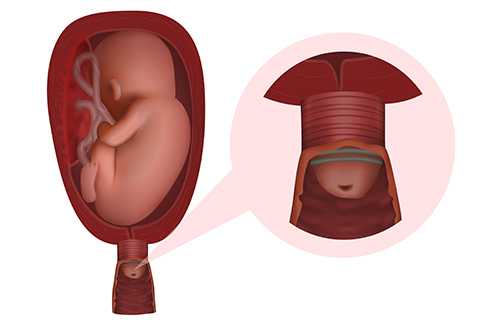
- If you undergo an Essure, it is imperative you use another form of contraception until confirmation of tubal occlusion. The HSG must be performed 3 months after surgery.
- Urogynecology procedures and vaginal approach reconstructions/repairs will need 6 weeks of light activity (no lifting >10 lbs) and abstaining from intercourse.
- All open abdominal surgeries can have an expectation of 6 weeks post-operative recovery time. Some surgeons may give you an abdominal binder, which will help with support moving around. This should be worn while moving about and should be put on snug, but not restrictive. The On Q pump is a form of continuous pain medicine delivered through 1 or 2 small tubes through the skin. It provides pain management for 3 days post-operatively. You will be instructed how to remove it during your hospital stay if the On Q is applicable to you.
For pre- and post-operative detailed timeline, please see the following surgical guide.

Oral pain medicines will be given to you at your preoperative visit so they may be filled and at your bedside when you return home from surgery. You may also get a prescription for medicines to take preoperatively the night before. In general, you should not drive post-operatively while you are still taking narcotics.
When to call
Postoperatively, notify your surgeon if you have pain that is not controlled by pain medicines, nausea and vomiting, fever of 101.0 in the first 2 weeks, purulent discharge, bleeding or any drainage from the incision site or vaginal bleeding in which you soak >1 pad/hr for two hours straight or inability to void for 4-6 hours. We will want to see you 3-4 weeks postoperatively.
Our Locations
- NORTHSIDE OFFICE
 404-252-1137
404-252-1137
- EAST COBB OFFICE
404-252-1137
- JOHNS CREEK OFFICE
404-252-1137
- NORTHSIDE FORSYTH OFFICE
404-252-1137
Let's stay in touch
Our monthly newsletter keeps you up-to-date on healthy lifestyle, latest news, and our practice.