

Genetic Screening and Testing
We live in exciting times and as a result of advances in genetic detection techniques parents have a wide array of choices for genetic testing of their pregnancy. Your choice of testing is personal and depends on your individual desires and your risk factors. The explanations found below will help you with your decision.
There are screening and diagnostic tests. How sure do you want to be? Is less than 100% “good enough”? That is the difference between a “screening” test, which gives you a likelihood of their being a problem versus knowing your baby’s chromosomes for sure.
Before you obtain any testing you need to answer the question: Would this information affect how I manage my pregnancy?
Screening tests used to be reserved for “low risk” women under age 35. The definitive and slightly more risky tests were offered to women at high risk for carrying a baby with a chromosomal abnormality and women over the age of 35. Nowadays, the high degree of accuracy in detecting fetal chromosomal abnormalities with the new screening tests means that many if not most women over age 35 opt for these tests as a first line. The diagnostic tests, which carry some risk to the pregnancy, are not pursued unless screening tests indicate a problem.
All women, regardless of age, are offered diagnostic testing if screening tests suggest an abnormality.
Screening tests
NT-first trimester screen
An ultrasound of the fetus measuring the nuchal translucency (thickness of scruff of the fetus’ neck) combined with blood from mother (free Beta hCG and PAPP-A). It is a way to detect for an increased risk of fetal cardiac and growth issues as well as chromosomal abnormalities. Currently, it is the only screening test that is available to evaluate multiple gestation pregnancies (twins/triplets/etc.) that are non biologic (donor egg or surrogate).
- Detection rate: 91% with a false positive rate of 2-5% for T21, and a 95% detection rate for T18/13 with a false positive rate of 0.3%
- Performed: 11 to 13 6/7 weeks
- Risk: none known to mother or fetus
- Results: less than 7 days
Fetal DNA in maternal serum testing:
Fetal DNA can now be detected and analyzed from a sample of maternal blood. It allows us to evaluate fetal chromosomes for specific disorders (T21/T18/T13) with an extremely high degree of accuracy and a low false positive rate (less than 1 in 1000) all with no risk to the pregnancy. Non-biologic (donor egg or surrogate) pregnancies can be accurately tested as well as multiple gestation pregnancies that are biologic. Non-biologic multiple gestation pregnancies cannot be tested at the present time. Fetal sex chromosome abnormalities can also be evaluated with a high degree of accuracy (99%) however the false positive rate is increased.
- Detection rate: >99% for T21, 97% for T18 and slightly lower for T13. Overall, false positive rate is 0.1%
- Performed: Anytime after 10 weeks
- Risk: none known to the mother or fetus
- Results: 7 to 10 days
Level II Ultrasound
More stringent ultrasound focusing on markers for chromosomal problems
- Detection rate: varies, likely 30-50%
- Performed: 18-22 weeks
- Risk: none known to mother or fetus
- Results: available immediately
At this point with the advances in genetic testing, we feel that a Harmony test in concert with an NT evaluation and a later second ultrasound evaluation looking for more subtle structural abnormalities provides the patient and her family with the highest level of evaluation with NO RISK to the pregnancy.
Diagnostic Tests
Chorionic Villus Sampling (CVS)
Involvesobtaining placental tissue through the cervix or abdomen. Does not evaluate structural abnormalities
- Detection rate: 97 to 100%
- Performed: 9 to 12 weeks
- Risk: fetal loss approximately 1/100 (1%)
- Results: 7 to 10 days
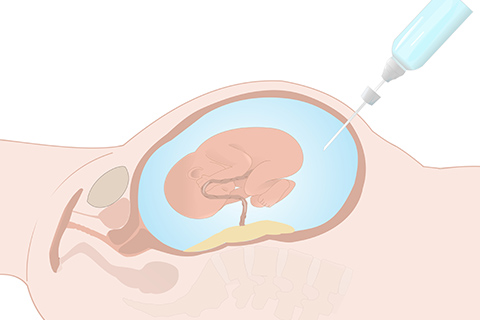
Amniocentesis
Obtain fluid from around the fetus by placing a needle through mother’s abdomen. Chromosomal evaluation only, does not evaluate structural abnormalities.
- Detection rate: close to 100%
- Performed: 16 to 18 weeks
- Risk: fetal loss approximately 1 in 200 (0.5%)
- Results: available in 10 to 14 days
Down’s Syndrome represents most couples’ primary genetic concern because this in one of the commonest chromosomal abnormalities that can survive to live birth. Your chance of having a baby with Down’s syndrome at age 25 is 1/1,250, at age 30 is 1/1000, at age 35 is 1/400 and at age 40 is 1/100. The majority of Down’s syndrome children are born to women under age 35 because more babies are born to younger women.
Now that you have read about the different tests and their benefits and drawbacks it is time to make a decision.
Please know that there is no requirement to obtain any test. If the results of the test would not affect your management or approach to your pregnancy then don’t feel compelled to do any testing. If you would want to know or if it would affect your approach to your pregnancy then you should pursue some level of testing.
For those aged less than 35 years and otherwise low risk individuals the standard of care is to be offered the AFP4 screening test. However, given the clear advantages of the newer tests both in detection and accuracy, all without risk to the fetus the vast majority of patients now choose the NT screening in conjunction with the fetal DNA test (Harmony). It can be performed before the end of the first trimester and is far more accurate.
For those age 35 years or older at delivery or otherwise high-risk individuals it is standard of care to offer an amniocentesis however many of our patients are choosing the screening package of tests, which carry the benefit of no risk to their pregnancy, first. Those couples have decided that the 99+% certainty that the NT test/Fetal DNA combination will detect an abnormality is “good enough” for them.


Let's stay in touch
Our monthly newsletter keeps you up-to-date on healthy lifestyle, latest news, and our practice.